
Effect of Sacubitril-Valsartan on Patient Reported Health Status in an Advanced Heart Failure Clinic
ABSTRACT
Background
Quality of life (QOL) is reduced in patients with heart failure with reduced ejection fraction (HFrEF). The Kansas City Cardiomyopathy Questionnaire 12 (KCCQ-12) is a validated self-assessment QOL tool for HFrEF. Sacubitril-valsartan was shown to statistically improve QOL when compared to enalapril in the PARADIGM-HF (Prospective Comparison of ARNI with ACE inhibitor to Determine Impact on Global Mortality and Morbidity in Heart Failure) trial. Real-world data is limited.
Objective
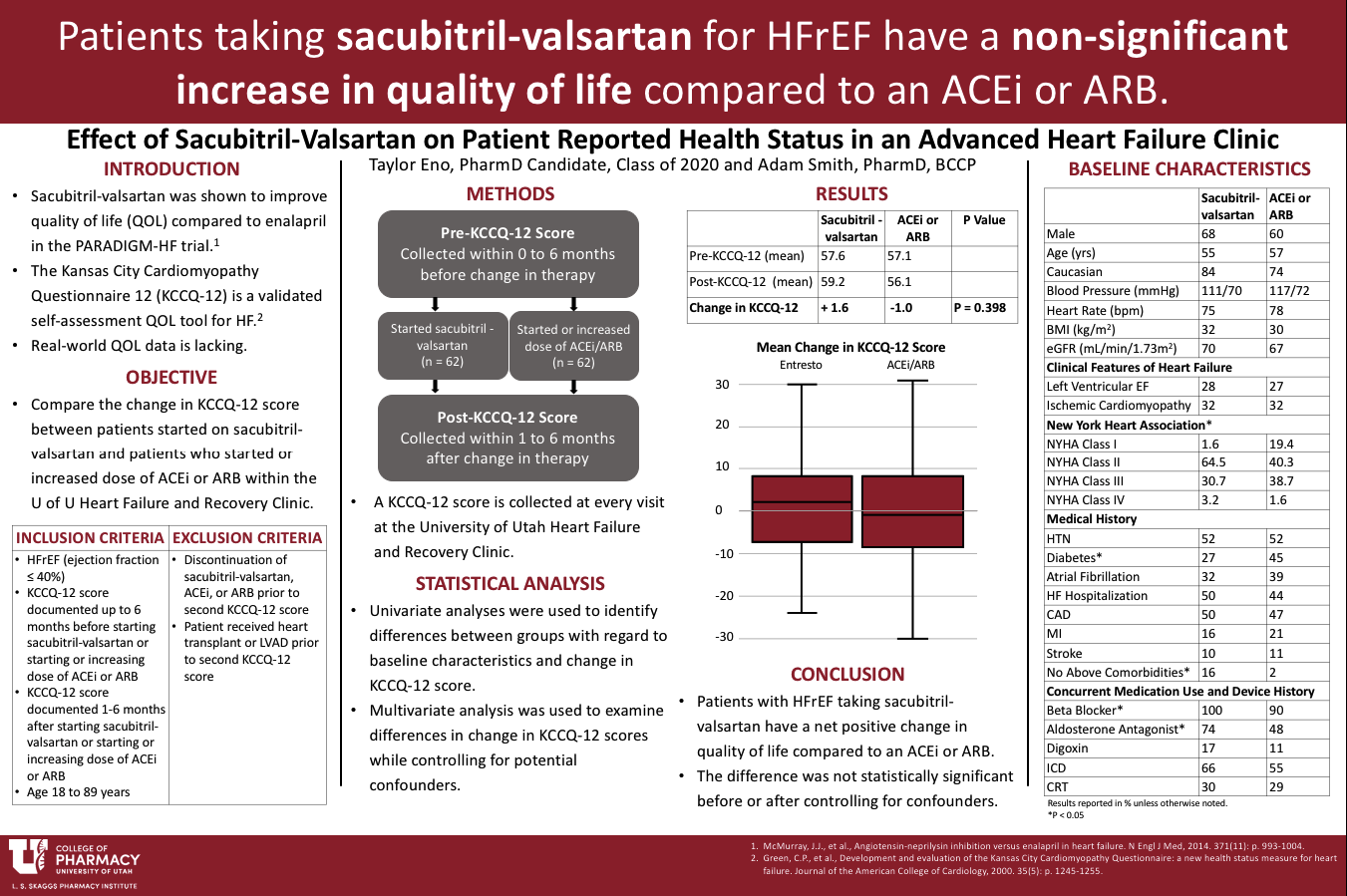
This study compared changes in KCCQ-12 score between patients started on sacubitril-valsartan and patients who started or increased dose of ACEi or ARB within the University of Utah Heart Failure and Recovery Clinic from January 1, 2016 to December 31, 2018.
Methods
Patients prescribed sacubitril-valsartan or who started/increased their dose of ACEi or ARB, with left ventricular ejection fraction ≤40% were identified. Included patients have a KCCQ-12 score recorded 0-6 months prior to and 1-6 months after the therapy change. Patient characteristics were obtained through chart review. The primary outcome is change in KCCQ-12 score. Regression analysis was used to determine if any variables affected the outcome.
Results
The mean change in KCCQ-12 score for the sacubitril-valsartan and the ACEi/ARB group was 1.6 and -1.0, respectively (p = 0.40). After controlling for differences in baseline characteristics and clinically relevant variables in a multivariate regression, there was no significant difference in KCCQ-12 between the two groups.
Conclusions
Patients starting sacubitril-valsartan had a non-significant increase in KCCQ-12 score when compared to patients that started/increased an ACEi or ARB.
Published in College of Pharmacy, Virtual Poster Session Spring 2020
Given the non-significant difference, do you think it is worth using one over the other for any other reasons? Is one cheaper or safer? Is there not enough evidence to say one way or the other? Nice work!
Hi Dr. Henchey,
Sacubitril/valsartan has proven mortality benefits over ACEi/ARB (PARADIGM-HF trial). Even though it did not improve quality of life, I think that because quality of life did not decrease and was even a little better than the ACEi/ARB group plus the added mortality benefit, sacubitril/valsartan is definitely worth using.
Thanks for asking!
Taylor
Really interesting study concept! I wonder what your results would be if you followed these patients for a year? I’m curious to see if the QoL results would be different!
Thanks! I wonder that also. If I could go back and do the study again, I would probably make the second KCCQ be within 6 months to 1 year instead of 1 to 6 months. I think that would give us a better idea of what the results would be over time.
Great work Taylor! How big was the improved QoL for the previous research? Is yours of similar magnitude and just not statistically different due to sample size? Or is there a lesser magnitude improvement in your study relative to the prior work? Also, could it be that your patients, given that they’re seen at a major medical center and have close follow up and care, don’t have as much room for improvement? I’m curious, if there are differences between your findings and the others that are perhaps driven by certain aspects underlying the QoL assessment.
Hi Dr. Keefe, thanks for your interest! The previous research that has been done had larger improvements in quality of life but was of similar magnitude to mine (i.e. sacubitril/valsartan improvement was about 2.5x the control group). There was a study that was recently published that used a large registry of heart failure patients and included a lot more patients than I was able to. They saw a statistically significant difference, so my small sample size could definitely be contributing to the nonsignificant result.
Your point about patients being seen at large medical center is valid. These patients are sick enough that their heart failure is no longer managed by a primary care provider and they are seen in a specialty clinic. Furthermore, when I was chart reviewing, I noticed that a lot of the patients received very close follow up care immediately following a hospitalization for heart failure. This could have meant that their recorded QOL scores during the time frame that I was looking at were actually worse than they might have been at a different point in time. Following the patients for a longer time period may have given me better results.