
Poulsen Mckayla
Descriptive Analysis of Anticoagulation Therapy Following Lung Transplantation
April 29, 2020 in College of Pharmacy, Virtual Poster Session Spring 2020
ABSTRACT
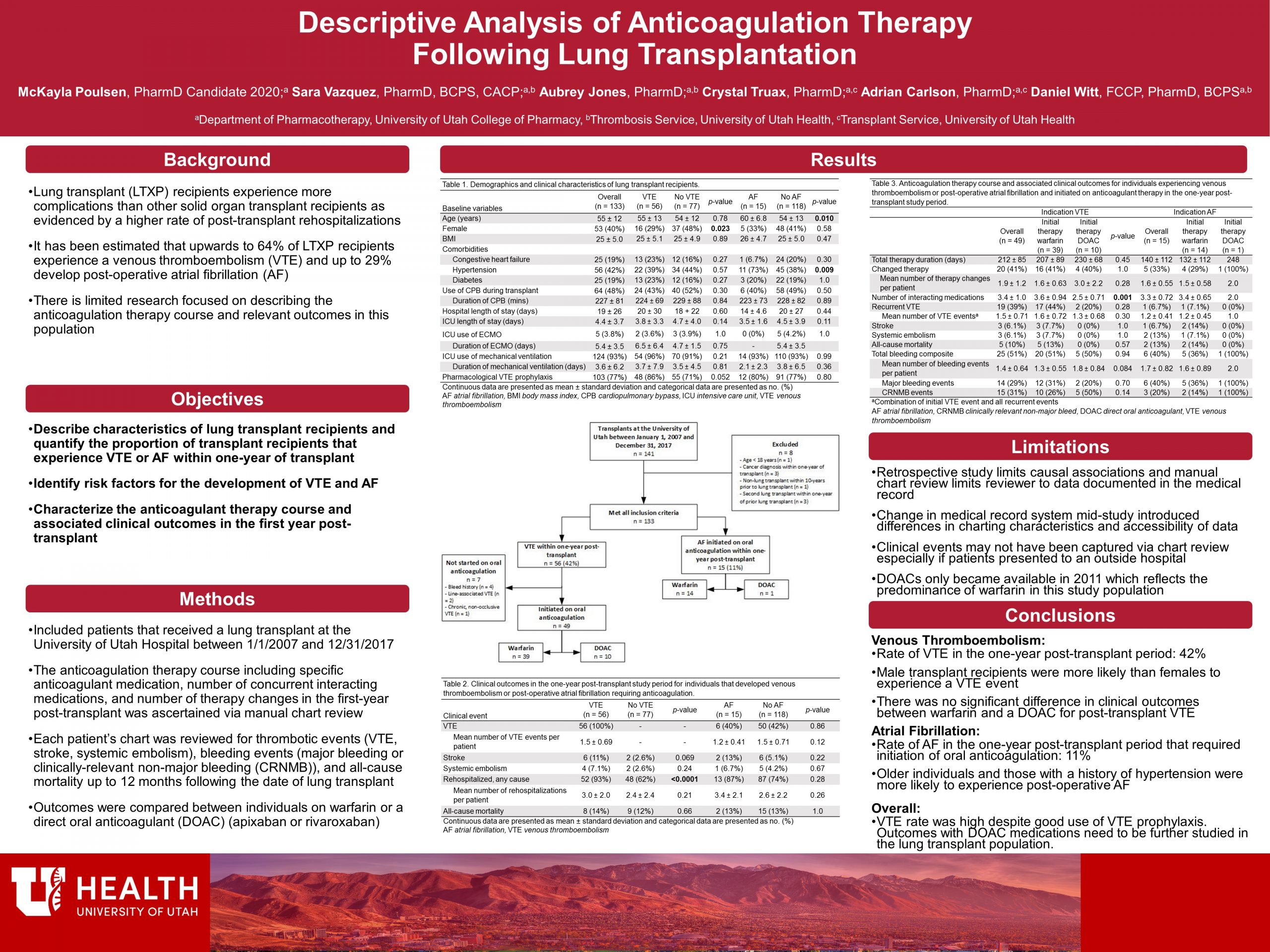
Background: Improved understanding of the clinical course of anticoagulated patients post-lung transplant may improve the prevention and management of thromboembolism and bleeding in this patient population.
Methods: This single-center, retrospective descriptive study analyzed patients who received a lung transplant at the University of Utah Hospital between 01/01/2007 and 12/31/2017. The study population was assessed for basic demographic characteristics, risk factors for and development of venous thromboembolism (VTE) or atrial fibrillation (AF), and anticoagulant therapy course. Clinical outcomes of interest included recurrent VTE, stroke, systemic embolism, all-cause mortality, bleeding, and rehospitalization.
Results: During the study period, 133 patients received lung transplantation and were eligible for inclusion. Of those, 42% experienced a VTE in the first year post-transplant. Male sex was a risk factor for the development of post-transplant VTE (p=0.023). Of those experiencing VTE, 49 were initiated on anticoagulation, with 39 (80%) on warfarin and 10 (20%) on a DOAC. Rehospitalization (p< 0.0001) and any bleeding (p=0.001) were more common in patients that experienced a VTE as compared to those who did not.
Fifteen (11%) patients developed AF and began anticoagulation during the first post-transplant year. History of hypertension (p=0.009) and older age (p=0.010) were risk factors for the development of AF. All patients but one were initiated on warfarin, the other on a DOAC, and were more likely to develop major bleeding as compared to those without AF (p=0.019). There were no statistically significant differences in clinical outcomes between those started on warfarin versus a DOAC in the VTE or AF subgroups.
Conclusions: VTE and bleeding are both common occurrences in the lung transplant population. Additional studies are needed to determine the best anticoagulation therapy course to minimize these outcomes.