
Testing Novel Steroid-Targeting Therapies for Tourette Syndrome in Transgenic Mouse Models
Abstract
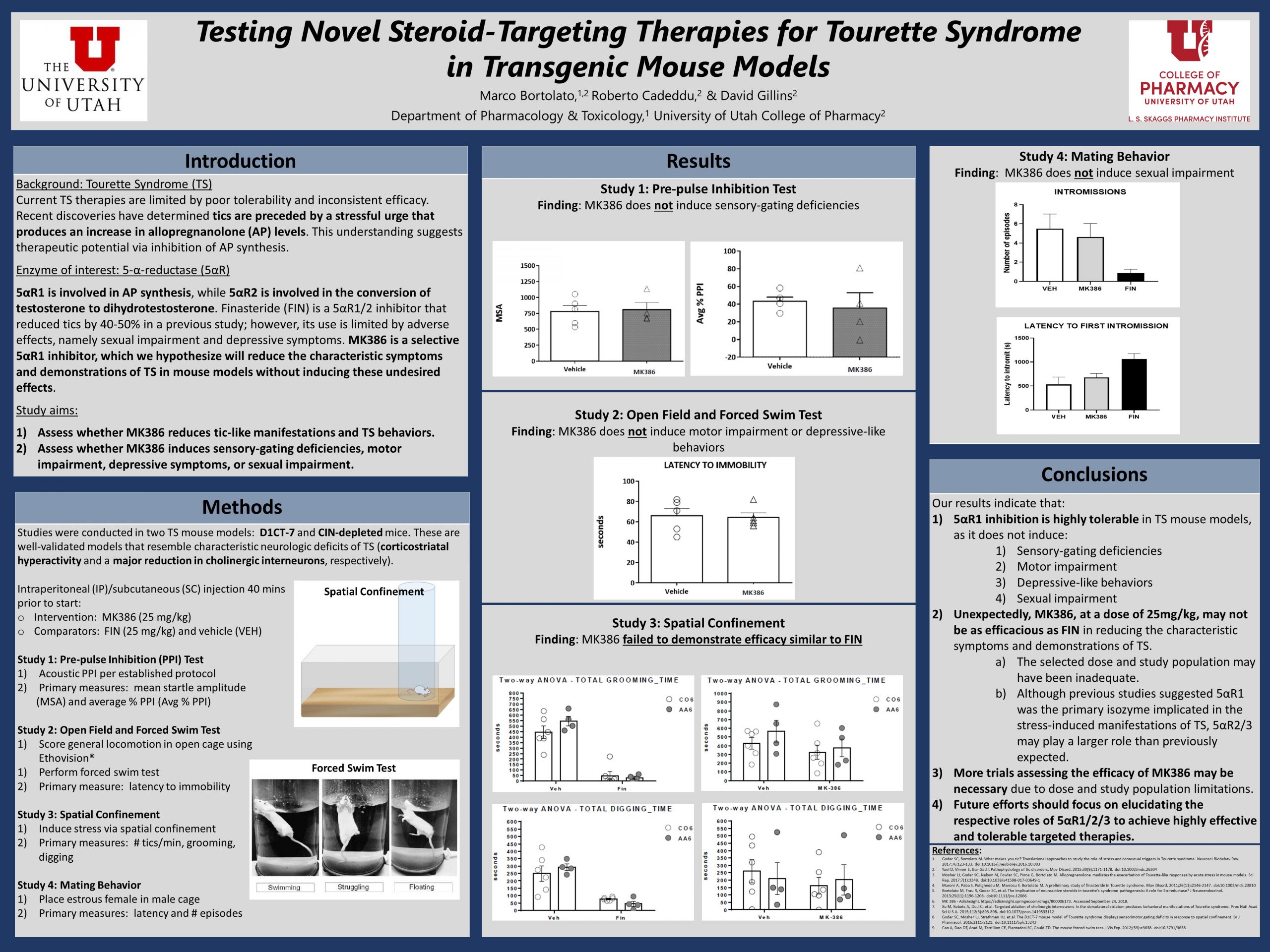
Tic management in Tourette syndrome (TS) is a significant challenge as available pharmacotherapies have limited efficacy and troubling adverse effects. Recent discoveries indicate that stress-induced production of the neurosteroid allopregnanolone (AP) plays a critical role in facilitating tic emergence. Finasteride (FIN), a non-selective AP synthesis inhibitor, has been demonstrated to substantially decrease tic frequency; however, it’s lack of selectivity often leads to adverse effects. This suggests therapeutic potential for a highly selective inhibitor of the main isozyme that produces AP, such as MK386. Our objective was to determine whether 1) MK386 reduces tics in TS mouse models without 2) inducing significant adverse effects. Studies were conducted in adult male wild-type mice (C57BL6/J) and transgenic mouse models (D1CT-7 and CIN-depleted mice). Mice were divided among treatment groups and administered MK386, FIN, or a solvent vehicle. A series of tests were performed to assess tolerability and effectiveness, including acoustic pre-pulse inhibition, open field observation, forced swim, and spatial confinement. Data was collected by a trained observer and analyses were conducted to determine the statistical difference between treatment groups. We found that treatment with MK386 does not induce sensory-gating deficiencies, motor impairment, depressive-like behaviors, or sexual impairment; however, our findings also indicate that MK386, at a dose of 25 mg/kg, fails to significantly reduce tics in TS.
Do you know if the lab is planning to look at higher doses, since you mention it may have been too low? Or are there other options that are also more selective than finasteride, but different from MK386?
There have been discussions about potentially testing higher doses of MK in the future; however, over the past year or so, the team has focused a lot of its efforts on another selective option, isoallopregnanolone (which inhibits the effects of allopregnanolone on GABA-A receptors – see Cole Warburton’s poster), as it was found to produce more promising results. There still exists the potential that the MK dose was simply too low. We originally planned to test multiple doses, but due to some setbacks we were unable to do so. I think it would still be a good idea to explore MK further down the road.
David, beautiful study and beautiful poster. Your results are quite convincing, but I appreciate your point about the dose potentially not being maximal. How did you decide on the MK386 dose? Are there independent measures of the 5AR1 inhibition that you could use to assess whether the drug at the doses given is effectively inducing the effect on 5AR1 activity that you seek?
Thank you! We originally planned to test 3 doses: 25, 50, and 100 mg/kg. Due to the high cost of MK386 and other setbacks, we decided it wasn’t feasible to test the higher doses at this time. I believe we decided on these doses as a starting point because similar doses were used in previous phase I/II clinical trials for acne and BPH. One independent measure we could utilize in future studies is to directly measure allopregnanolone levels in the brain. This would allow us to determine if the tested dose effectively suppresses AP biosynthesis through 5AR1 inhibition. If we test multiple doses and find that AP levels are still elevated, we could conclude with more certainty that another 5AR isozyme is playing a more significant role than we expected in AP production.