Introduction: Patients are treated for refractory status epilepticus (RSE) with either midazolam, propofol, or pentobarbital, in addition to other concomitant anti-epileptic drugs (AEDs). Pentobarbital has a lower RSE treatment failure rate than midazolam or propofol, but patients often experience serious adverse effects (AEs) when pentobarbital is used, leading providers to reserve this medication as last-line therapy. We present a series of patients treated within the University of Utah health system for RSE with pentobarbital and discuss the adverse effects experienced by these cases.
Methods: This retrospective study included adult patients treated for RSE with pentobarbital between July 2014 and June 2019. The primary aims of this study were to describe the incidence of AEs and to evaluate the AE management methods at U of U Hospital. AEs were graded according to the severity and reported if management required hospitalization and advanced treatment. AE management methods were described.
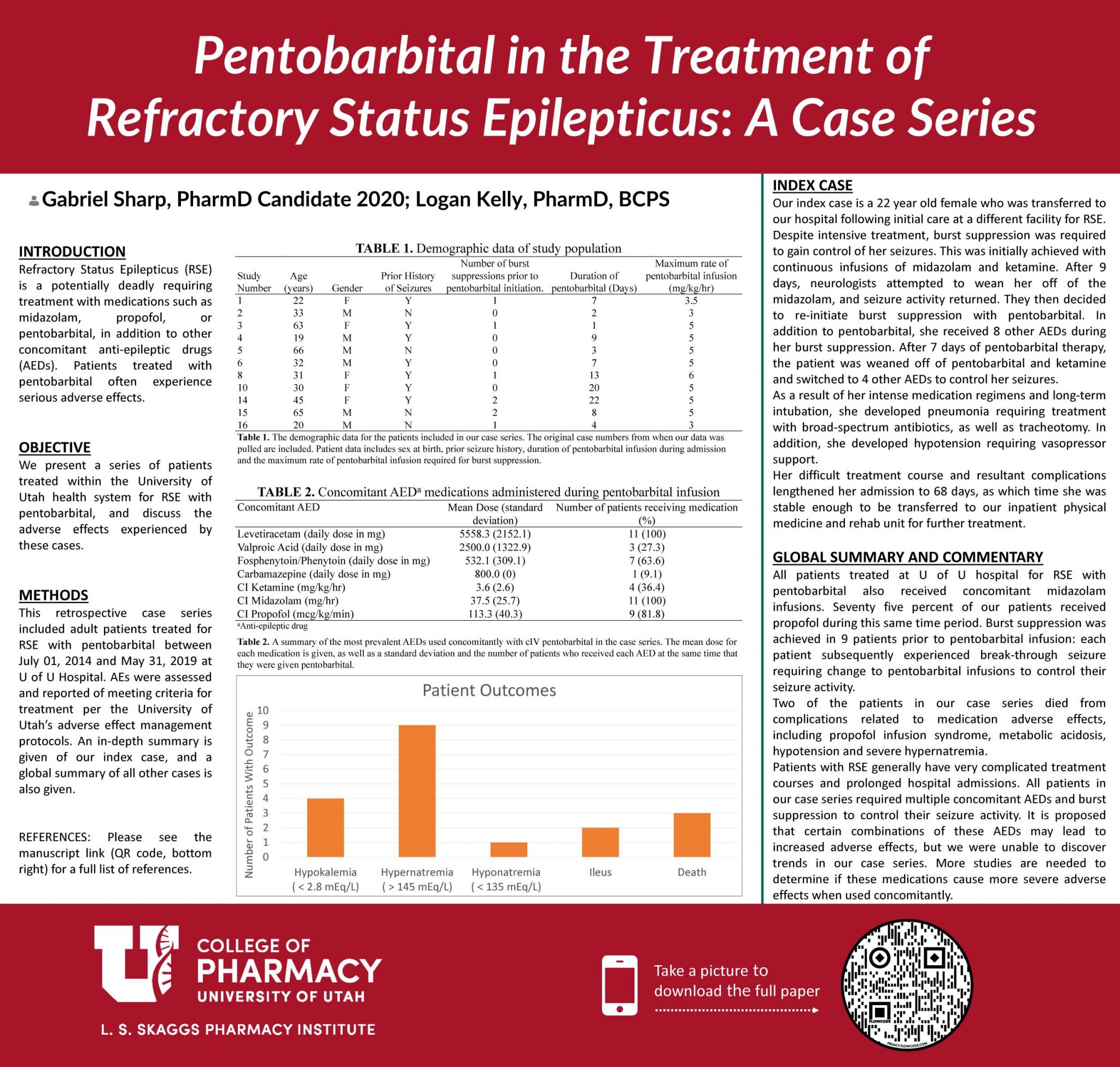
Results and Discussion: AEs experienced by the patients were reported. 3 of the patients died from adverse effects related to the AED medication administration. Only 2 patients experienced ileus that required treatment. Adverse effects did not appear to be associated with the maximum dose of pentobarbital that a patient received during admission. Most of the patients treated with pentobarbital experienced hyponatremia during their hospital admission.

Gabe, very nice poster. I like how you link to the full paper through the QR code. I’m curious to what extent you think that it is the use of pentobarbital itself vs. simply the severity of the cases requiring pentobarbital that leads to the adverse events?
Dr. Keefe,
Thank you for your comment. The continuous infusion AED medications used in controlling seizures are known to lead to adverse effects, the most common being hypotension in these patients. This particular adverse effect appears to be directly related to the medication administration, such as pentobarbital. In fact in this article, cited here: https://pubmed.ncbi.nlm.nih.gov/11903460/, they show that pentobarbital in their study population had a consistently higher rate of hypotension in RSE patients than those treated with the other medications. Our particular case series made it impossible to see if this bore true for us as well.
I feel that some of the other adverse effects, such as dramatic sodium shifts, could be due in part to the severe condition itself. It is difficult to know this for sure, as there is no control population that doesn’t receive any medication.
Hi Gabe, great poster and interesting case series! In your summary you mention the hypothesis that different combinations of AEDs for RSE may lead to increased AEs. I’m not sure if you have this information, but did the adverse effects observed support this hypothesis (i.e., based on the exact combination of AEDs received and possible AEs of those AEDs)?
Thank you for your comment Dr. Heath. Due to the small sample size that we had in our case series, it is very difficult to see if specific medications contributed to a higher rate of specific AEs with pentobarbital. We were unable to confirm that there were more adverse effects in certain patients. In addition to this, the severity of the patients in our case series necessitated that most of them received the same medications at one point or another. There did not appear to be any correlation with the adverse effects and specific regimens that patients received.
Interesting topic. I’ll definitely check out your full manuscript- love the inclusion of the QR link.
Nice job on this project! This is a very difficult topic to review, but really important to evaluate.