ABSTRACT
Background
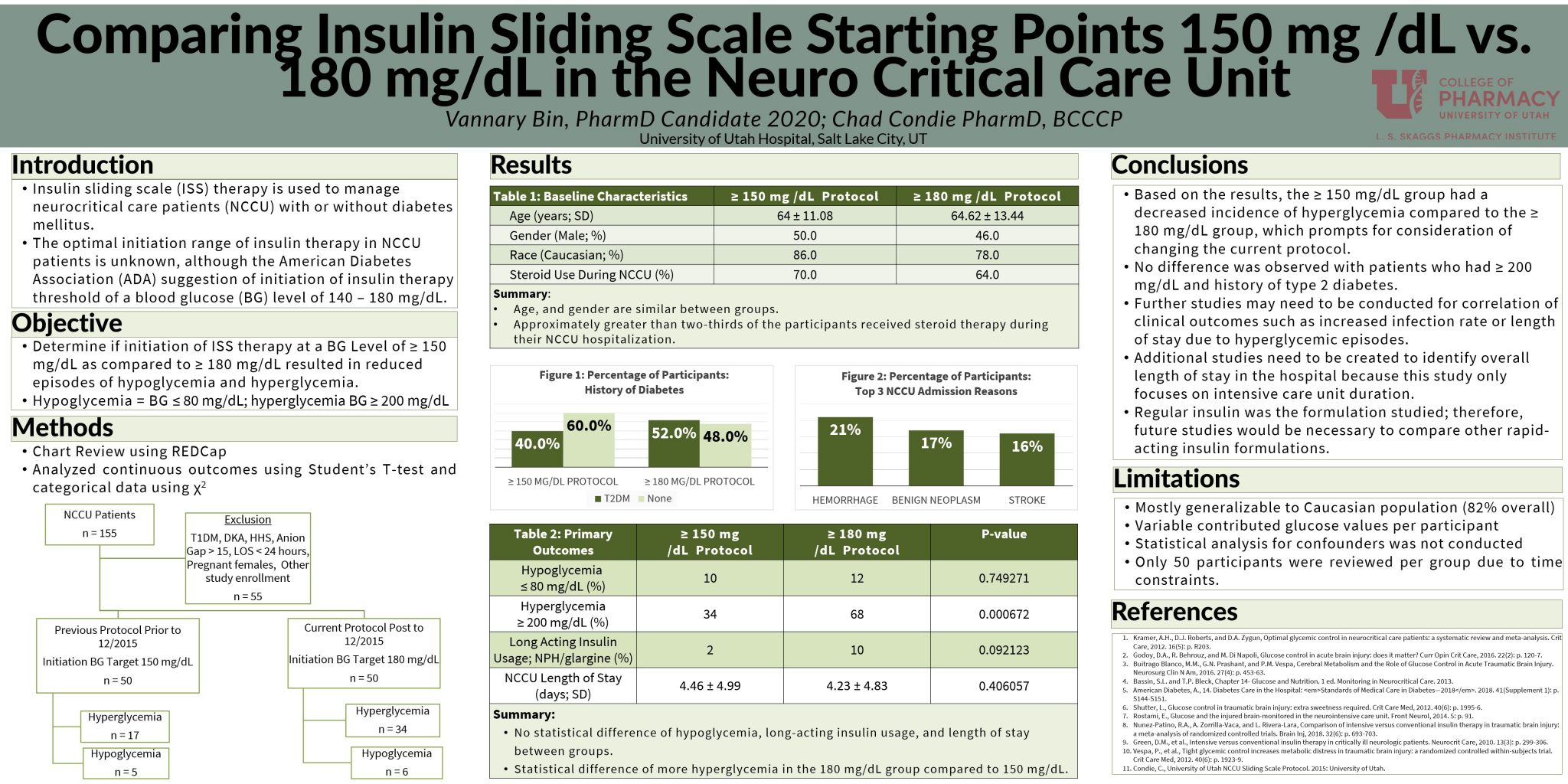
To provide better insulin sliding scale management, the University of Utah Hospital (UU) updated the neuroscience insulin sliding scale protocol to incorporate a higher hyperglycemia threshold of 180 mg/dL compared to previous blood glucose (BG) of 150 mg/dL. The previous and updated protocol are both within the American Diabetes Association (ADA) recommendation guidelines, yet it is unknown if this update has an increase or decrease effect regarding safety.
Objective
The primary objective of our study is to determine if initiating insulin sliding scale therapy among the UU Hospital neurocritical care patients at a BG level of ≥ 180 mg/dL compared to a BG of ≥ 150 mg/dL reduced hyperglycemia or hypoglycemia events and decreased the length of stay.
Methods
This is a descriptive study conducted as a retrospective chart review performed at a single-center, UU Hospital.
Results
Hypoglycemia episodes have no statistical difference (p=0.749271) between both groups. Whereas more hyperglycemia events in the ≥180 mg/dL group compared to the ≥ 150 mg/dL group with a statistical difference (p=0.000672). Long-acting insulin usage resulted in no difference (p=0.092123). The length of stay was 0.23 less days in the ≥ 180 mg/dL group, but was not of statistical significance (p = 0.406057).
Conclusion
Based on the results, the ≥ 150 mg/dL group had a decreased incidence of hyperglycemia compared to the ≥ 180 mg/dL group, which prompts for consideration of changing the current protocol. Further studies may need to be conducted for correlation of clinical outcomes such as increased infection rate or length of stay due to hyperglycemic episodes. Regular insulin was the formulation studied; therefore, future studies would be necessary to compare other rapid-acting insulin formulations.