Abstract:
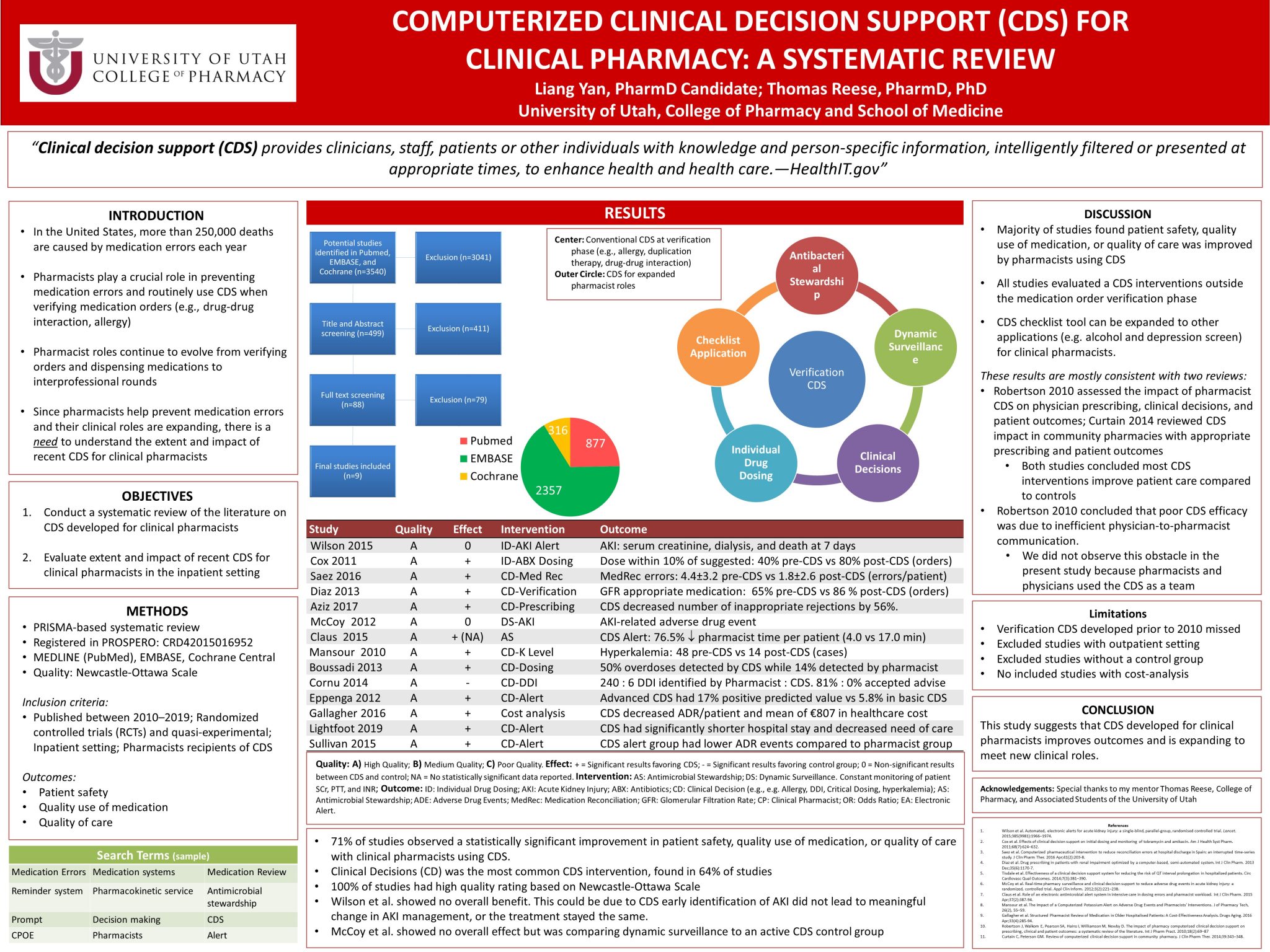
Introduction: In the United States, more than 250,000 deaths are caused annually by medication errors. Pharmacists play a crucial role in preventing medication errors and optimizing pharmacotherapy. Moreover, clinical decision support (CDS) tools are continually developed to help clinicians improve medication safety. While pharmacist roles are expanding, the vast majority of CDS has been targeted at prescribers. Our goal was to evaluate the literature to understand the impact of recent CDS targeted at clinical pharmacists.
Hypothesis: Recent CDS has been increasingly developed for clinical pharmacists in the inpatient setting to reduce medication errors and optimize pharmacotherapy.
Study design: Systematic Review
Methods: We searched MEDLINE, EMBASE, and Cochrane Central databases from 2010 to 2019. We included randomized controlled trials (RCTs) and quasi-experimental studies evaluating a CDS tool developed for clinical pharmacists at inpatient setting. The primary outcome of our analysis was the impact of CDS on patient safety, quality use of medication, and quality of care. Outcomes were scored as positive, negative, or neutral. The secondary outcome was the proportion of CDS developed for tasks other than medication order verification. Additionally, we assessed study quality using Newcastle-Ottawa Scale.
Results: Our search resulted in 3542 studies. Following title-abstract screening (498) and full-text review (87), 13 studies met our inclusion criteria. Among 13 studies, 7 were RCT and 6 were quasi-experimental study designs. We found CDS interventions significantly improved patient safety (5), quality use of medication (4), and quality of care (4). Fives studies (38%) evaluated a CDS tool developed for an expanded role of clinical pharmacists.
Conclusion: Our results show that CDS may support clinical pharmacists in preventing medication errors and optimizing pharmacotherapy. We found that CDS tools have been developed for pharmacist roles outside order verification, which suggests healthcare institutions are beginning to recognize pharmacists as leaders in safe and effective pharmacotherapy.

Thanks for an interesting poster. I wonder, did you find (or are you looking into) any attributes present in the 71% of CDS that improved patient outcomes (and not in the remaining 29%) which may inform how to successfully build a CDS? Also, if cross-provider communication is an obstacle to successful use of CDS, do you have any suggestions for ensuring that the information from the CDS is properly distributed to all providers?
Hi, thank you for interested in my poster. For the CDS that improved patient outcomes, there wasn’t a description on how CDS is built to properly incorporate into their study, other than the CDS should report patient data the study is interested (for example CDS has to report SCr in Wilson et al. or it has to report antibiotic dosing in Cox et al).
As for the cross-provider communication, my suggestion is to design a CDS that can relay information/question from the inquirer to the responder. In current EPIC system, the provider will have to send their question to the pharmacy team themselves, which I anticipate is what’s happening with cross-provider communication: the provider has to know who can answer their question before they send it. It would be more efficiently if a CDS can conduct this automatically, or at least give a step-wised approach to find the right person who can answer the question.
Nice study. Thank you for sharing. One issue with CDS for clinical pharmacists is that often times, prescribers see similar information earlier in the medication ordering process. Can you comment on if this was reported by any of the studies that were included in your final sample? Thanks.
Hi, thank you for sharing on a prescriber point of view. As for my study, part of our inclusion criteria is that the CDS had to be designed towards pharmacists. There wasn’t any prescriber information that I’ve noticed or discussed for CDS application.
In majority of the study, the ordering process by the prescriber has already been completed, and then comes the CDS for pharmacists as an alert on possible DDI or inappropriate prescribing. On rare occasion, the CDS will help with dosing calculation which is also done by pharmacists after the drug was ordered by the prescriber. Due to this, we did not include on how CDS effected prescriber in this study.
Liang, well done study and nicely presented poster. You present your work in a very scholarly manner. I hope that this was a good experience for you!
Hi Dr. Keefe, thank you very much. This PharmD project has been a great experience for me and definitely expends my knowledge and add on to my future career.
Liang – congratulations for your nice job. I enjoyed reading your poster. The readers will learn more about your review if you describe study design and the comparator of each study. It looks like some of them are pre-post design, while some are RCT with a control group. Understanding the design and comparator will help us better justify the conclusion that “CDS improves outcomes”.
Regarding quality assessment tool, I wonder why NOS is used in non-observational study. I think NOS Is not appropriate for RCT. Have you considered risk of bias (Cochrane) for RCT?
Thank you Dr. Chaiyakunparuk. Yes this study incorporated a mix of study designs. This is because we intend to examine how CDS that target pharmacists has changed over the past decade. If we were to put a limit on trial designs, this would shrink even further and not meet what we intend to examine.
The reason we used NOS is because this quality assessment tool is designed to look at quality of the study in a systematic review that has a mix of study designs. We would consider a different tool if our study only look at one types of studies.