Purpose: Asthma self-management education (ASME) is a fundamental component of asthma management that improves asthma outcomes and generates cost savings related to a reduction in unnecessary health care use. Pharmacists can play a key role in providing ASME services and improving asthma outcomes for their patients. Key informant interviews were conducted with pharmacists performing ASME services within Utah pharmacies. This allowed us to better understand what ASME practices are currently used within the state. These findings will be used to further evaluate and improve Utah ASME strategies in addition to providing a foundation for a future pharmacist-led ASME program.
Methods: Key informant interviews were performed with eight Utah pharmacists who reported to regularly provide ASME services. Interview questions focused on ASME methods, reimbursement incentives and barriers. Interview audio was transcribed and then analyzed thematically using a qualitative descriptive approach.
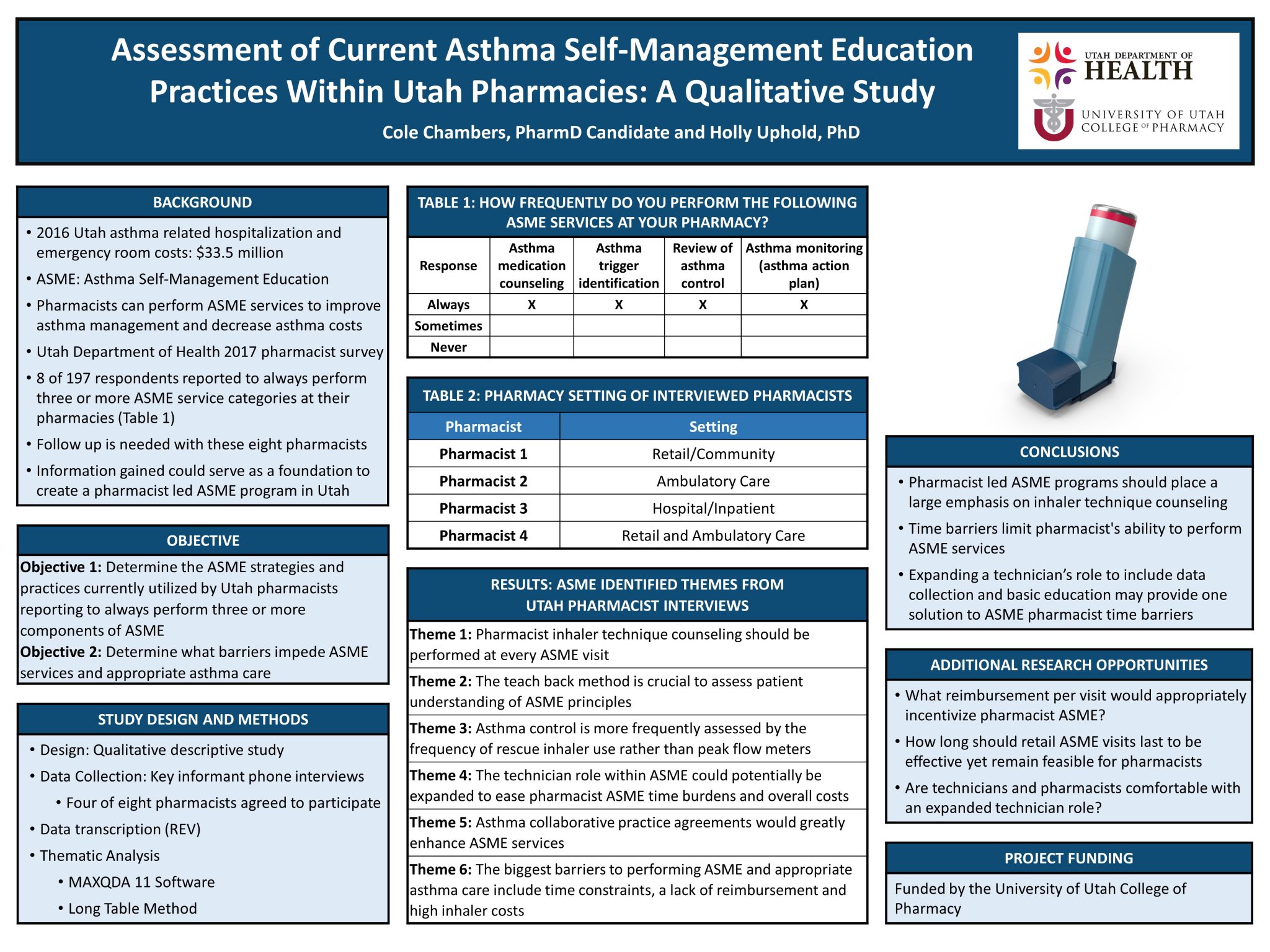
Results: Five common themes were identified as critical components of ASME practices, including: the importance of inhaler counseling at every visit, the importance of the teach back method to assess patient understanding, widespread pharmacist use of rescue inhaler usage to assess asthma control, the importance of collaborative practice agreements within ASME, and the potential use and expanded role of pharmacy technicians within ASME. Barriers to ASME services included time, lack of reimbursement, and high inhaler costs.
Conclusion: This study identified several key strategies for pharmacists to perform effective and feasible ASME. Future ASME programs should focus on incorporating components of inhaler technique counseling while maximizing the role of pharmacy technicians to overcome ASME time barriers.

Pharmacists will provide teaching each visit? That is great.
Hi Jane! Yes, however at this point in time what we found is that regular pharmacist teaching and patient assessment rarely happen in the retail space. Most often patients will receive initial counseling on their inhaler (if they ask or accept counseling to start with) and then they go their way with little structured follow up. Our hope is that with the data gathered from this project, in the near future the Utah Department of Health could create a standardized pharmacist led asthma education program that empowers pharmacists to follow up with their patients and to provide their education in a more structured way to ensure that the patients are getting all the education and care that they need. This project lays out some of the key focus points on which a future program should build.
Nicely done, Cole! I find it interesting that only 4/8 who initially responded agreed to the follow up. Do you have any sense of why that is?
Hi Dr. Keefe! Thank you for the opportunity to provide a little more clarification. Our initial 8 pharmacist candidates were survey respondents from the year 2017 (previous student’s PharmD project). That 2017 survey was carried out online and was extremely convenient for the pharmacists to complete. For our project, we then tried to reach these pharmacists again in 2019 for follow up, two years following the original survey. Unfortunately, only 4 pharmacists replied to our contact attempts via email and phone. No one that we were able to make contact with declined to participate in our study. Perhaps some of the other pharmacists who did not reply had changed employment, contact information or moved since 2017. We did offer $50 Amazon gift cards to participating pharmacists which I thought was a pretty good incentive.
One more thing, I found the point that asthma control is better assessed through use of rescue inhaler (I’m assuming either patient self-report of frequency or frequency of refills) vs. peak flow meter interesting. It seems it might be possible to develop a computer algorithm that could flag patients with more frequent refills of rescue inhalers as a way to alert the pharmacist to work more closely with that patient?
Yes, I completely agree. In fact, this is one area of ASME where I believe retail pharmacists have an advantage over other settings. If a patient comes in to fill their inhaler earlier than they should, insurance will often reject the claim and the pharmacy and pharmacist can then ask the patient for more information regarding the patient’s albuterol use. Our survey was completed with pharmacists from all different pharmacy settings and most of the pharmacists reported to just take the patient’s word for how often they use their inhaler, but the added claims data is a nice advantage for retail pharmacists.
I love the way your poster proposes the need for further research into a piloted expanded technician role in order to understand how that could benefit pharmacy!
Thanks Michael, I think a lot of technician’s could play a larger role in gathering data from patients. They could use a standardized questionnaire to cover a lot of information that pharmacists would normally be asking. Once that questionnaire is completed, it could be passed along to the pharmacist who could then focus their time and efforts on only the areas of concern. Thanks for your comment! Hope all is well!
I agree! Thank you, Cole!
Hi Cole, I’m sorry if this ends up appearing as a repeat comment – apparently I submitted a comment before, but it is not appearing now.
Anyway, great work on your poster! Your presentation of the information is excellent.
Can you elaborate on why you selected the pharmacists always completing 3/4 ASMEs for your sample? I wonder if these pharmacists perspectives would differ from the other pharmacists in the original survey (perhaps particularly regarding objective 2, barriers to ASME).
Cole- Nice work for poster and manuscript too. I wonder if you can address the issue of sample size. Do you think interviewing 4 pharmacists would be enough? How can we know whether these would be enough? Do we need a sample size calculation?
Nice work Cole! It important to publish on the value of pharmacist led education on the use of inhalers, I know Dr Young is well award of this!