Objective
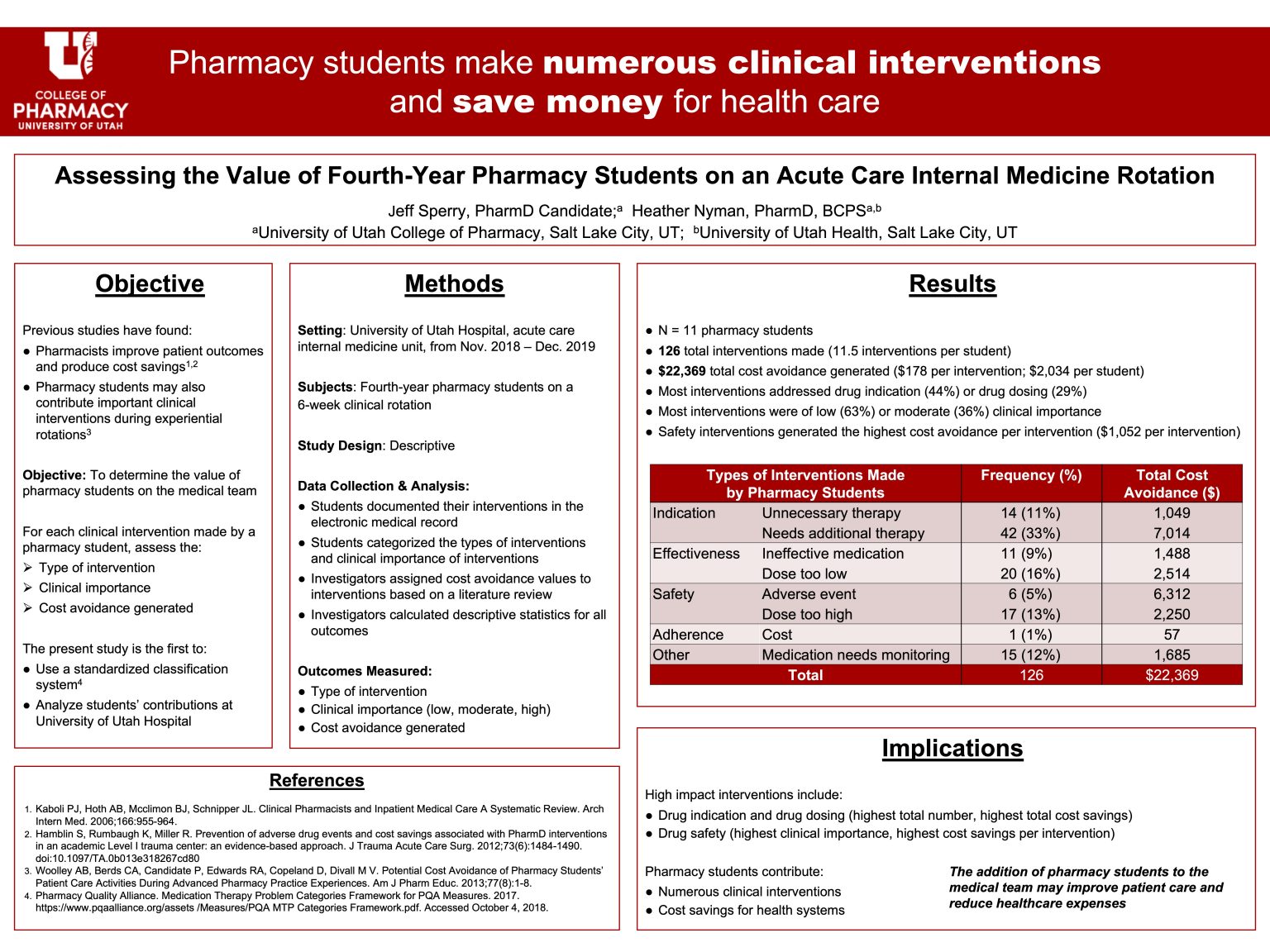
To catalog the clinical interventions (CI) made by fourth-year pharmacy students using a standardized categorization framework, describe the students’ perceived clinical importance of interventions, and estimate the cost avoidance produced by interventions.
Methods
In this descriptive study, fourth-year pharmacy students documented their CIs made during a 6-week acute care internal medicine rotation at University of Utah Hospital. Interventions were categorized by type according to a standardized system and classified as low, moderate, or high in terms of perceived clinical importance by the student. Based on a literature search, interventions were assigned a cost avoidance dollar value, and an estimated total cost avoidance generated by student interventions was calculated.
Results
Eleven pharmacy students made a total of 126 interventions from November 1, 2018 through December 31, 2019, which produced an estimated $22,369.19 in total cost avoidance. Each student made an average of 11.5 interventions (range: 5 – 22) during their six-week rotation, or 0.44 interventions per day (range: 0.19 – 0.76) and 0.34 interventions per patient (range: 0.12 – 0.70). CIs regarding preventive therapy (19.8%), untreated condition (13.5%), and dose too low (12.7%) were the most common types of interventions recorded. The majority of CIs were of low (62.7%) or moderate (35.7%) in terms of perceived clinical importance.
Implications
Pharmacy students are valuable members of the healthcare team. They made a substantial number of CIs that represent important cost-savings for the healthcare system, but further research is needed to continue characterizing the value of pharmacy’s contribution to patient care.

Great job Jeff! This project was really interesting and reassuring as a student! I think it would be equally interesting to see how this correlates with the opinions of healthcare providers that the students are interacting with. Does the team similarly find value in our interventions and the role we play in a patient’s care outside of saving a healthcare institution money? Maybe this has already been assessed? If not, it could be a neat comparator!
In the papers I read, I did not see any that reported data regarding the team’s perception of having a pharmacy student (other than the rate of how often they accepted or rejected their recommendations). I really like that idea though, and I agree that it would be interesting to see if they felt that having a pharmacy student was valuable.
Jeff, I liked the way you presented this data. Thanks for all of your work on this project!
Thank you Dr. Nyman for all of your help!
Great poster, Jeff. What was one thing you learned as you worked on this project that you think will be helpful to you in the future?
I really liked that this project had me thinking deeply about the value of pharmacy. What do pharmacists provide that is absolutely essential? What is our highest point of contribution? And I think in order to answer that, we need solid documentation to produce good data. I think the self-report nature of this study was quite difficult. It really relied upon the student remembering to document their interventions and documenting them accurately. In order to better capture the activities of students (and of pharmacists) and to better demonstrate our value, I think it would be ideal if we had better systems like an automated data collection tool integrated into the normal pharmacist workflow to help track some of these things, and then finding the most effective ways to communicate those findings.
Jeff, Nicely done! The poster is clear, with the data concisely presented and interpreted. I’m curious how one calculates a cost savings for the intervention that the medication needs monitoring?
For medication monitoring, we decided to put it in an “Other” category because monitoring something like INR for patients on warfarin, for example, ensures both efficacy (that they’re adequately anticoagulated) and safety (that they’re not at a huge risk of bleeding), so it didn’t really fit cleanly into just the “Efficacy” category or “Safety” category. But it’s always kind of tricky estimating cost avoidance. By monitoring INR, you could potentially prevent a serious safety event. You would multiply the cost of the serious safety event times the probability of it happening. These are just made up numbers as an example, but say the cost of a serious bleeding event requiring hospitalization is $5,000 per occurrence, and this happens in 5% of patients taking warfarin when they do not have adequate INR monitoring. So over the course of 100 patients for whom you intervene and add INR monitoring, you could potentially prevent 5 episodes of severe bleeding (and save 5 x $5,000 = $25,000 total per 100 patients, which averages to $250 per 1 patient, that is, you save an average of $250 each time you make an intervention to add INR monitoring).
Wow, what powerful findings! Pharmacy students rock! Great cost savings and interventions.
Thank you Dr. Lim for stopping by to see our posters!
Amazing job Jeff! I think this really solidifies the value pharmacists have on interprofessional teams. We make large contributions, especially in medication management (indication, doses) as you have presented. Thank you for presenting this data!
Thank you Ashley! It is definitely reassuring to see how we can have an impact on patient care.
Jeff,
Interesting study and well-done poster. I liked the analyses and the conclusion that pharmacy students save the hospital money (and perhaps patient lives). What do you think would be the next study that should be done to carry this research forward another step?
I think it would be interesting to look at associating specific pharmacy interventions or activities with patient-centered outcomes like length of stay, morbidity, mortality, readmission rates, and patient satisfaction. These could also be great ways to communicate impact on patient care, and because reimbursement is more often being tied to quality of care, demonstrating that pharmacists/students impact these measures would additionally help a hospital financially. Other interesting things to investigate could be the patient’s perspective and the medical team’s perspective (whether they thought it was helpful or valuable having a pharmacy student).
I think this is interesting and matches what we are doing on the outpatient side. I wonder if the cost savings might actually be higher because depending on the medication and their cost, it could change things. Good work – nice quant/qual combo with the other poster.
Yes I think the cost savings would definitely depend on the type of medication. The numbers used here are more like averages for each category, but a more accurate estimate would consider the specific drug and the specific adverse event that was prevented for each intervention, for example, but that would also be harder to do. But errors prevented for very expensive drugs would clearly save more money.
Hi Jeff, great study! I’d heard that it was in progress and have been awaiting the results. You’ve collected and analyzed some tangible data that pharmacy students bring value to patient care, as well as managing costs. Although total cost avoidance is a useful metric, I wonder if there are other metrics that may lend themselves better to statistical analysis?
I think the ideal situation for a true statistical analysis would be to use a control group. For example, medical teams would be randomly assigned a pharmacy student, and we compare the performance of those medical teams with a pharmacy student vs those without a pharmacy student (or those teams with a pharmacist vs those without a pharmacist). Outcomes such as length of stay, morbidity, mortality, readmission rates, and patient satisfaction would be interesting to compare, although I think we would need a larger sample size to detect a significant difference.
Jeff- great project! I was wondering how you counted the total number of interventions per rotation. Were these the interventions that were made by the students without prompting from preceptors and if so how did you determine this while collecting the data? Or did you include all interventions made by a student regardless of preceptor involvement?
One of the data points that we collected was the source of the recommendation (the APPE student, a pharmacy resident or pharmacist preceptor, someone else on the medical team). We only included interventions that primarily originated with the APPE student in this analysis.
Nice job on this project!
Thank you for stopping by and taking a look at our posters!