ABSTRACT
Purpose: Limited evidence exists regarding managing recurrent venous thromboembolism (VTE) that occurs during ongoing anticoagulation therapy. We aimed to describe patient characteristics, drug therapy management, and outcomes of patients with VTE recurrence during ongoing anticoagulant therapy.
Methods: Adult patients admitted between January 2017 and December 2018 with a diagnosis of recurrent VTE during ongoing anticoagulant therapy were included. Manual medical record reviews were performed to summarize information on patient characteristics, recurrent VTE therapy, and associated outcomes.
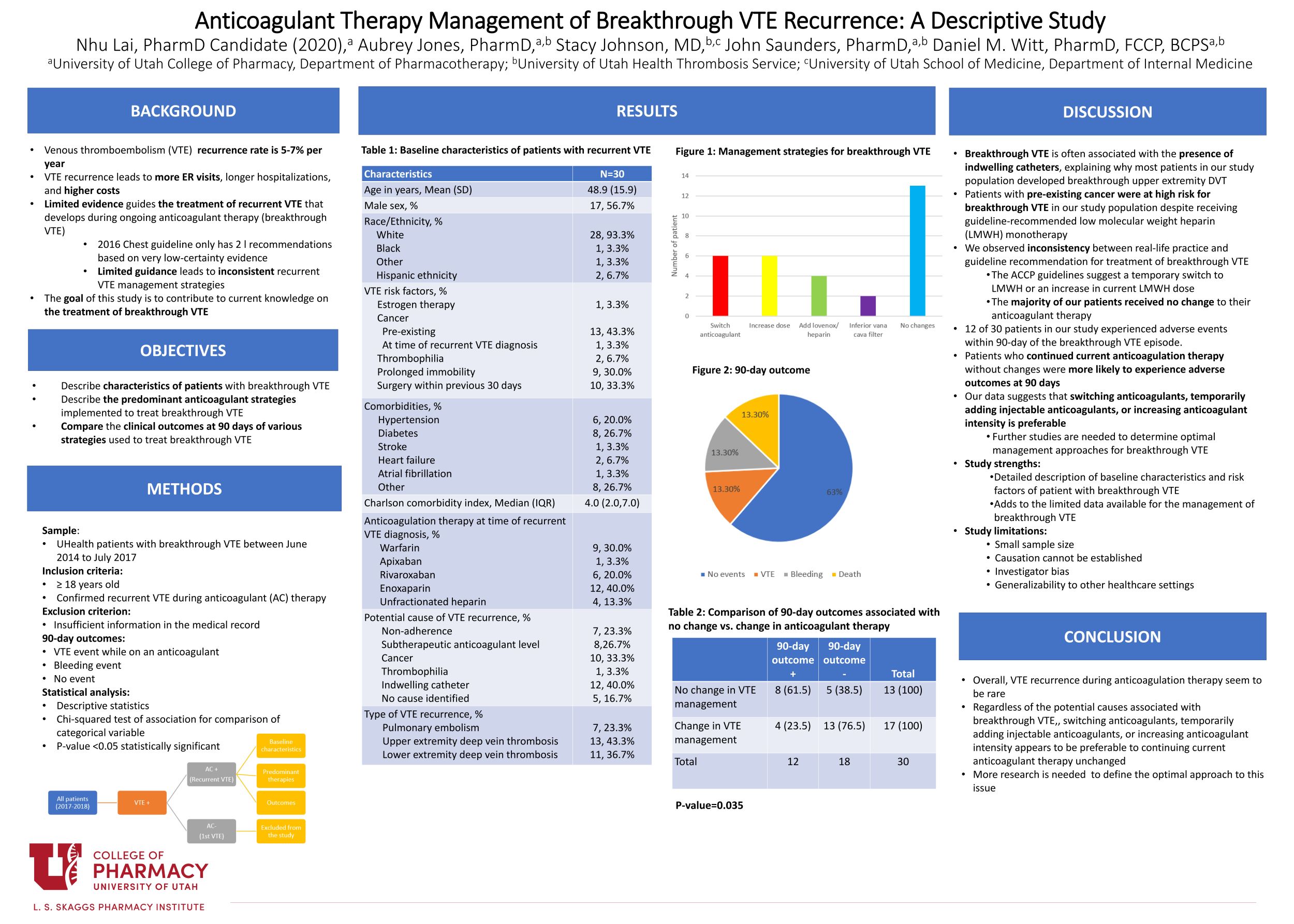
Results: We identified 30 episodes of VTE recurrence. Mean age was 48.9 (15.9) years, 56.7% were male, and 93.3% were White. Common VTE risk factors included cancer (46.6%), recent surgery (33.3%), and prolonged immobility (30.0%). At the time of recurrent VTE, 40% were receiving enoxaparin, 30.0% warfarin, and 23.3% direct oral anticoagulants. Potential causes for VTE recurrence included indwelling catheters (40.0%), cancer (33.3%), subtherapeutic anticoagulation (26.7%), and nonadherence (23.3%). Recurrent VTE management strategies included switching anticoagulants (26.7%), increasing the anticoagulant dose (20.0%), temporarily adding enoxaparin or unfractionated heparin (13.3%), or no change in anticoagulation therapy (43.3%). Only 4 adverse 90-day outcome occurred among the 17 patients who received anticoagulant therapy changes in response to VTE recurrence, whereas 8 adverse outcomes occurred in the 13 patients who received no change in anticoagulation therapy in response to a recurrent VTE episode (P-value 0.035).
Conclusions: Regardless of the potential causes associated with recurrent VTE during anticoagulation therapy, switching anticoagulants, temporarily adding injectable anticoagulants, or increasing anticoagulant intensity appears to be preferable to continuing current anticoagulant therapy unchanged.

Very interesting research and results of treatments in that one cannot always wait to see if the treatment will work but change it to get better results.
I agree. We were surprised when most of our patients did not have any changes to their therapy. But when we look at the outcomes closely, our data suggest that patients who received changes in their anticoagulant therapy appeared to have a better outcomes.
Hello Nhu. Very nice poster and study. The results, of course, scare me a bit, given the adverse outcomes, but I guess it is good to know that the recurrent VTE itself was a rare event. I am a bit unclear about your Table 2. When you write “90-day outcome +” does that mean that there was an event or that the 90 outcome was positive (i.e., no event). Based on your conclusions, I assume the “+” means there was an adverse outcome, whereas the “-” means there was not, but I wasn’t sure from Table 2 itself.
Hi Dr. Keefe,
Thank you for your comment. I could see how my wording could be quite ambiguous. The “90-day outcome +” in table 2 means there was an event (either a VTE episode or a bleeding event) that occurred within the 90-day period.
Nhu! Nice job. Very interesting results – and very timely. I just saw a patient who had a recurrent VTE while on warfarin, and based on these results I would likely recommend lovenox or a higher goal range for a short period instead of changing nothing. Not at all what we expected. But its good to re-affirm that recurrent VTEs while on anticoagulation really are quite rare.
Hi Dr. Jones,
I agree. The results we got were very interesting. But wow! How cool! I’m glad that the result of this study is applicable to your recent patient.
Thank you so much for all your help with my project.
Strong work, Nhu! I’m a little curious, do you know if the individual anticoagulants (e.g. rivaroxaban, apixaban, etc.) dosed appropriately at the time of the VTE recurrence?
Thank you so much for your comment, Angie. Unfortunately, I don’t have data on the individual anticoagulant. But overall, out of 30 patients included in our study, there were 8 patients who were at a subtherapeutic level at the time of the VTE recurrence.
Nhu, your poster looks great. Thank you for being responsive to the feedback we provided. You note that more research is needed to define the optimal approach to managing breakthrough VTE, if you were going to design a study to provide additional information, how would you go about it?
Hi Dr. Witt,
Thank you for the comment and all your feedback throughout this project.
As for your question regarding the next step- based on our data, it appears that overall change in anticoagulation is preferrable in managing patients with a breakthrough VTE recurrence. I think the next appropriate step would be to look closely at outcomes associated with each therapy change so that we can have a better idea of which therapy strategy would be optimal. The independent variable could be therapy changes, such as a temporary switch to a LMWH (if so, for how long), an increase in current anticoagulant dose, an additional therapy, would be optimal. The dependent variable could be the 90-day outcomes (as defined in this study) associated with each therapy change.
In addition, as VTE recurrence is rare, I think we could extend our study time period to increase the sample size.
Hi Nhu,
Great job on your poster and all the research that went into it- Sure exited you’ll be finishing soon! Congratulations
Thank you Judy
Nhu, good job! I am sure this project required a lot of medical record review.